.jpg)
The Problem of Autistic Identity
- 3 days ago
- 9 min read

Diagnosis, Comorbidity, and the Question of What Makes Us Who We Are
Before discussing autistic identity, it is necessary to clarify several terms that will be used throughout this article.
Identity refers to the qualities, beliefs, personality traits, social roles, and affiliations that define a person or a group. It may include characteristics such as nationality, sex, profession, values, political or religious beliefs, and membership in particular communities. For example, a person may describe themselves as "a teacher, a parent, and a musician."
Identity is not fixed. Some aspects remain relatively stable throughout life, whereas others change as individuals encounter new experiences, environments, and social roles. Identity serves as a framework through which people understand themselves, develop a sense of belonging, establish values, and make everyday decisions.
A useful distinction can be made between self-identity and social identity.
Self-identity refers to a person's own understanding of who they are. It is the internal perception through which individuals define themselves and make sense of their experiences. Different people emphasise different aspects of themselves: one person may define themselves primarily through family, religion, and personal interests, while another may place greater importance on career, ethnicity, or political beliefs.
Social identity refers to a person's identity as derived from membership in social groups. These groups may be based on factors such as age, ethnicity, nationality, language, religion, socioeconomic status, disability, or sexual orientation. Some social identities are chosen, while others are assigned by society.
The distinction can be summarised simply:
Identity is how a person is recognised or categorised in the social world.
Self-identity is how a person understands and defines themselves.
Social identity is the part of identity that arises from group membership.
These dimensions of identity constantly interact. Society provides labels, expectations, and roles that can influence how individuals see themselves, while self-identity can shape which labels people accept, reject, or reinterpret.
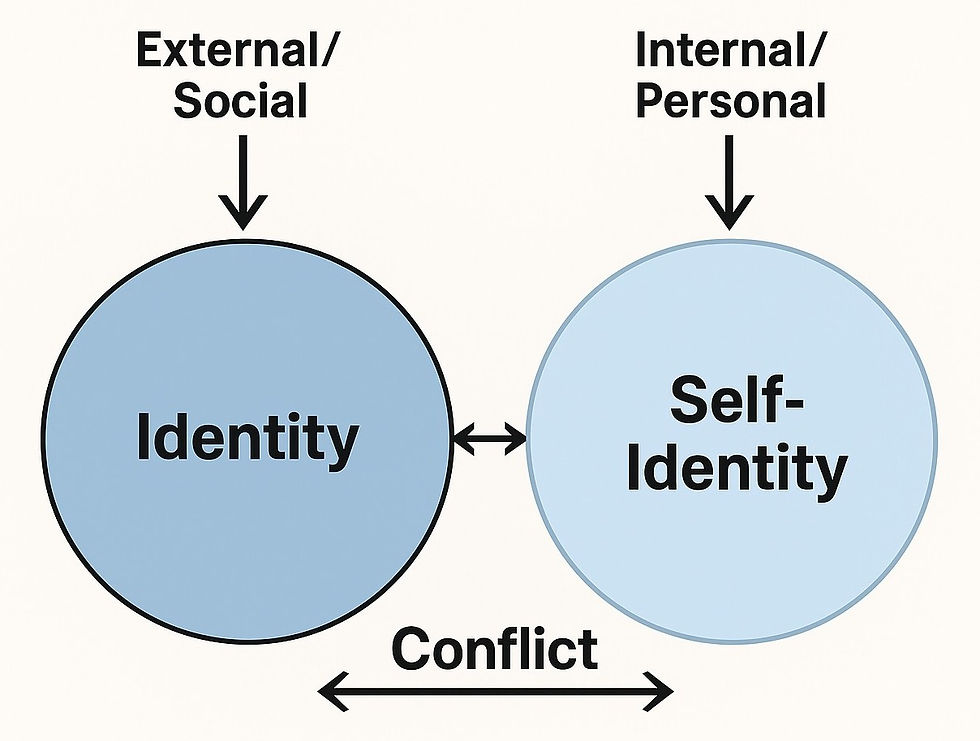
Tensions may arise when external categorisations conflict with a person's self-understanding, or when an individual's self-concept differs substantially from how others perceive them.[1]
What Is an “Autistic Identity”?
Autism as Diagnosis and Autism as Identity
Identity plays a central role in contemporary discussions of autism. For many individuals, diagnosed or self-diagnosed in late teens or adulthood, autism is not merely a clinical category but a framework for self-understanding, community, and belonging.
The relationship between diagnosis and identity raises important philosophical questions.
A medical diagnosis is a classificatory construct: it groups observable traits, behaviours, or physiological patterns into a coherent category for clinical and research purposes. It is descriptive and pragmatic. It does not, in itself, make an ontological claim about the essence of a person.
Autism/ASD is a heterogeneous clinical category, comprising a group of autism subtypes which have little in common with each other, e.g., some autistic individuals are high-functioning and accomplished, others self-harm and non-verbal (Choi et al. 2022; Némorin et al. 2025; Whiteley et al. 2025).[2]
For many autistic individuals, adopting an identity-first perspective is not about medicalisation but about reclaiming difference from deficit-based narratives. In this context, “autistic” is not merely a diagnostic label but a meaningful expression of lived experience, cognition, and community.
However, the move from diagnosis to identity raises a broader question: should a clinical classification be regarded as an identity category? If a diagnosis defines identity, then consistency would require that all diagnoses do so.
The Problem of Diagnostic Attribution [3]
The practice of self-diagnosis is spreading rapidly. An increasing number of people identify as autistic without an official assessment, relying instead on online materials, personal stories, and popular symptom checklists. However, the very term "self-diagnosis" is misleading.
A diagnosis is not merely a matter of assigning a label to certain experiences; rather, it is the outcome of a structured clinical process conducted by qualified professionals. While individuals may interpret their own conditions, the use of psychiatric diagnoses outside the framework of such a process carries no official validity (Davis 2022). More accurately, what is occurring is personal appropriation (Davis 2010): the selective adoption of diagnostic categories to make sense of experience. Individuals draw on a mixture of sources—search engines, social media, anecdote—and reshape diagnostic criteria to fit their self-concept. Less appealing elements of clinical definitions tend to recede; more affirming ones are retained.
The DSM-5 significantly altered autism diagnostic criteria, merging separate categories such as Autistic disorder, Asperger's, childhood disintegrative disorder, and pervasive developmental disorder not otherwise specified (PDD-NOS)[4] into a single umbrella: Autism Spectrum Disorder. This change was aimed at streamlining the diagnosis and improving consistency. However, over a decade later, clinical accounts suggest it resulted in in thousands of adults, particularly those diagnosed in adulthood, being misdiagnosed with ASD despite no evidence of childhood onset or developmental symptoms.
The shift from DSM-IV to DSM-5 should have been supported by a clear and reliable method for handling diagnostic change. Instead, DSM-5 introduced a “grandfather clause”[5] that automatically converted DSM-IV diagnoses of Autistic Disorder, Asperger’s Disorder, and PDD-NOS into ASD.[6] As a consequence, someone who had already been diagnosed with DSM-IV PDD-NOS were automatically given a diagnosis of ASD after the publication of DSM-5, even though PDD-NOS was not an “autistic disorder”.
Interestingly, such an ASD diagnosis would be ‘inherited’ even if the current symptomatology would suggest a different diagnosis or even no diagnosis at all under the DSM-5 diagnostic criteria.[7] Clinical accounts suggest it resulted in thousands of adults, particularly those diagnosed in adulthood, being misdiagnosed with ASD despite no evidence of childhood onset or developmental symptoms.
Dr. Jonathan Shedler, Clinical Psychologist, known for his work in personality pathology, has warned that clinicians are increasingly bypassing psychodynamic understanding in favour of simplistic, checklist-driven labels: "The rise in autism diagnoses overlaps suspiciously with conditions like borderline personality disorder, avoidant personality disorder, and trauma histories. We’re mistaking defense mechanisms and relational trauma for neurodevelopmental difference.” (2023)
Thus, a conceptual tension remains. If identity is formulated in diagnostic categories because they profoundly shape perception, interaction, and daily life another question is: are self-diagnosed individuals qualified to differentiate between diagnoses or do they attribute one or two characteristics to autism from overlapping features in other conditions?
Dr. Sami Timimi, Child & Adolescent Psychiatrist (2022), who has written extensively about the over-pathologising of normal behavior, warns that many young people diagnosed with ASD would better be understood through psychosocial lenses, including trauma and attachment: "We are seeing autism as the new ‘one-size-fits-all’ label for anyone who feels different. The criteria are so vague that we’ve essentially medicalised personality diversity, trauma, and even introversion.”
Diagnostic manuals run to hundreds of pages, clinicians undergo years of training, and comprehensive assessments often involve multiple interviews, developmental histories, and differential diagnosis. Yet on social media, confidence in an autism diagnosis can sometimes emerge after a weekend of online content consumption.
Actually, anyone can self-diagnose as autistic because autistic traits can be present in individuals in the general population (Baron-Cohen et al. 2001; Ruzich et al. 2015; Moshirian Farahi, Leth-Steensen 2023; Zhang et al. 2024; Wu et al. 2025).
Many neurotypical individuals exhibit Broader Autism Phenotype (BAP)[8] – the expression of behavioral and cognitive dispositions similar to ASD themselves.(Bolton 1994; Piven et al. 1997)
The Problem of Trait Attribution
The first attribution problem concerns diagnosis itself: is the person autistic? The second is more subtle. Even when the diagnosis is correct, it remains unclear which aspects of experience are attributable to autism and which arise from other sources.
The question is not trivial. Autism rarely exists in isolation. Research consistently shows high rates of both physical and psychiatric comorbidity among autistic individuals. Conditions such as ADHD, anxiety disorders, depression, mood disorders, personality disorders, epilepsy, gastrointestinal disorders, allergies, and sleep disturbances occur at substantially higher rates in autistic populations than in the general population. Many autistic individuals experience more than one co-occurring condition simultaneously.[8]
In addition, a significant proportion of autistic individuals (50% - 55%) experience alexithymia – difficulty identifying and describing one's own emotions. Estimates vary across studies, but rates are substantially higher among autistic individuals than among non-autistic populations. Some researchers have argued that characteristics commonly attributed to autism, particularly in the domain of emotional awareness and empathy, may in some cases be better explained by alexithymia than by autism itself.
The problem becomes even more complex when symptom overlap is taken into account. Many characteristics commonly associated with autism are not unique to autism. Difficulties in social relationships, emotional instability, withdrawal from social interaction, intense interests, anxiety, and interpersonal misunderstandings may also occur in trauma-related conditions, mood disorders, anxiety disorders, personality disorders, and other psychiatric conditions.
The challenge, therefore, is one of attribution. When an autistic person experiences social difficulties, emotional dysregulation, interpersonal problems, anxiety, sensory sensitivities, rigid patterns of thinking, or interpersonal challenges, it is not always clear which of these experiences arise from autism itself, which stem from co-occurring conditions, and which reflect personality, life experiences, or environmental circumstances.
This distinction matters because identity claims frequently rely on causal assumptions. To identify a particular characteristic as "autistic" is to assume that autism is its primary source. Yet in the presence of extensive comorbidity and symptom overlap, such assumptions are not always easy to justify.
When autism (or autistic traits) coexist, for instance, with anxiety, BPD, alexithymia, and hikikomori tendencies, should identity expand accordingly? (making descriptive language increasingly layered). One might half-jokingly imagine increasingly elaborate formulations: the “obsessive-compulsive alexithymic AuBPDer with hikikomori tendencies”? Or, perhaps, the “anxiously alexithymic autistic NPDer with obsessive- compulsive and hikikomori tendencies”? And if additional conditions are present, should they be appended as well?
Taken to its logical conclusion, this approach quickly becomes unmanageable. The point is not to mock identity-based language, but to show its limits.
Many conditions—psychiatric and somatic—shape behaviour, temperament, and life trajectory. Diabetes, chronic pain, or anxiety disorders can profoundly influence daily existence. Yet we do not typically interpret them as defining personal essence and do not construct identity around each of them. The selective elevation of one diagnosis to identity status, while treating others as mere clinical add-ons, reveals an inconsistency and reflects social and cultural dynamics rather than philosophical coherence.
The question, therefore, is not whether autistic people are entitled to identify as autistic. Rather, it is whether the broad concept of an "autistic identity" accurately captures the origin of the characteristics, experiences, and personality traits that individuals attribute to autism.
*****
“And the moral of that is – ‘Be what you would seem to be’ – or, if you’d like it put more simply – ‘Never imagine yourself not to be otherwise than what it might appear to others that what you were or might have been was not otherwise than what you had been would have appeared to them to be otherwise.” (Lewis Carroll).

____________________
[1] Conflicts between self-perception and external categorisation are neither new nor unique to contemporary identity debates. Throughout history, individuals have sometimes understood themselves in ways that differed markedly from prevailing social or medical interpretations. The manner in which societies respond to such discrepancies has varied across time and cultures, ranging from attempts at correction or treatment to acceptance, accommodation, or affirmation. The appropriate response remains a subject of ongoing social, philosophical, and clinical debate.
[2] The manifestation of autistic symptoms varies greatly depending on factors such as the severity of the autistic condition, the developmental level, and the chronological age. Thus, ASD is meant to encompass a variety of conditions characterized by varying levels of symptoms severity—ranging from low (or even zero) to severe—that were previously considered as independent disorders, such as Early Infantile Autism, Childhood Autism, Kanner’s Autism, High-functioning Autism, Atypical Autism, Childhood Disintegrative Disorder, Asperger’s Disorder, and PDD-NOS (APA 2013).
[3] Attribution theory explores how we infer the causes of our own and other people’s behaviour in order to understand and predict the social world. It deals with how the social perceiver uses information to arrive at causal explanations for events. It examines what information is gathered and how it is combined to form a causal judgment (Fiske & Taylor 1991).
[4] In the ICD-10, PDD-NOS is classified as Atypical Autism (AA) under the code F84.9 (Pervasive developmental disorder, unspecified). This was a residual category used for individuals who did not meet the full, strict criteria for classic Childhood Autism (F84.0) or Asperger’s Syndrome (F84.5) or other specific PDDs but still exhibited significant challenges in communication, socialisation, or restricted behaviours.
[5] The “grandfather clause” is a provision in which an old rule continues to apply to some existing situations while a new rule will apply to all future cases.] Likewise, an individual that would now have no diagnosis at all (because he meets neither the ASD criteria nor the SPCD ones), would still be diagnosed with ASD if he had a DSM-IV diagnosis of PDD-NOS (Kim et al. 2014; Regier et al. 2013).
[6] At consultations regarding changes in DSM-5, many scholars and patients’ advocates have expressed their worries about the practical consequences of the DSM-5 revisions relating to ASD (Autistic Self Advocacy Network 2012; Greenberg, 2013; Ne’eman & Kapp, 2012). because losing an ASD diagnosis would imply the exclusion from a well-established network of organisations engaged in clinical services, healthcare assistance, education, employment, economic support, and research (Weismer et al. 2021).
[7] In addition, to autism diagnosis having been attributed through “inheritance”, there are others who were given PDD-NOS by mistake – a copyediting error: the DSM-IV put an ‘or’ instead of an ‘and’ among the diagnostic criteria of PDD-NOS. Hence, it was theoretically possible to diagnose someone with PDD-NOS in the absence of problems with social interaction (First & Pincus, 2002). This means that the grandfather clause did not only ‘fossilize’ an old diagnosis, but also an unintentionally mistaken one (Cooper 2015).
[8] The Broader Autism Phenotype (BAP) describes subclinical, autism-related traits that present in individuals who do not meet the full diagnostic criteria for (ASD). These milder traits often manifest in the non-autistic family members of autistic individuals and provide insight into the genetic and inherited nature of autism. The traits associated with the broader autism phenotype typically mirror the core diagnostic domains of autism but are milder and usually do not cause significant impairment in daily functioning.



Comments